Welcome to our community bulletin where we will publish articles of interest and relevance.
CoVivre-20. By now we are all needing to live in close quarters with those we share our homes. We are having to learn to adapt to each other’s daily routines without stumbling over others in the same house. We are having to cohabit in its truest sense. Each day we are all thinking of the days ahead when we can meet again, and move on. We must all progress from how we feel. To represent this new step in cohabitation and moving forwards in time, we have decided upon the title CoVivre-20 for our newsletter.
History of Osteopathy
Please click on the link on The Anatomy Lesson of Dr Nicolaes Tulp below
Rembrandt van Rijn, The Anatomy Lesson of Dr Nicolaes Tulp, 1632 (Mauritshuis, The Hague)
This group portrait by the young Rembrandt is a snapshot from medical history. A famous Amsterdam surgeon, Dr Nicolaes Tulp, performs a dissection in front of his guild. The corpse of a hanged criminal is laid out on a table. The skin of his left arm has been peeled back for Dr Tulp to explain its mechanics, showing how the muscles are attached to the bone by tendons. His colleagues look on with fascination and amazement, and one looks out at us, as if we are also present at the anatomy lesson.
This group portrait showcases the production of medical knowledge in the seventeenth century, a combination of received wisdom, as represented by the open book to the right, and first-hand observation, which is the purpose of the dissection. The Renaissance saw the birth of modern science, when empirical observation started to trump ancient texts and the authority of the church as a means to heal the sick.
OSTEOPATHY
So why osteopathy? I will start by sharing with you why I chose it as a lifestyle and a little about the history of the profession. After you have read this, we would love to hear why you chose osteopathy as your preferred therapy or any anecdotes you would like to share with the group.
The Anatomy Lesson of Dr Nicolaes Tulp reminds me of my early curiosity of how things worked in general. I was always more fascinated by the workings of a toy car by taking it apart than the laborious pleasure of pushing it around a track. I remember the excitement I felt as an eight-year-old when I handled a dead bird I found on a very hot balcony floor; the mechanics of stretching its wings out with its series of hinges and the systematic arrangements of the wing feathers was a real eureka moment. Dissecting pig’s hearts and frogs in Biology was equally fascinating to do, as was handling the carcass of a rabbit or chicken prior to being put in the oven! The fascination was not just the mechanics of how it all worked, but also of how it felt. Holding and handling parts captured my imagination.
When it came to choosing a career, the idea of being able to make things work again was high on my agenda. Amongst the various considerations, osteopathy had a unique attraction in the early 1980's: that of being alternative and fringe. It appealed to my sense of being quietly rebellious. So against all popular advice from teachers, I embarked on my training at the British School of Osteopathy, and never looked back!
The painting illustrated here links osteopathy to the pioneering work of Andreas Vesalius (a 16th Century Flemish anatomist), and indeed, surgeons of the Dutch Golden Age like Dr Tulp, whose contributions to the understanding of the body ultimately made non-interventive medicine possible.
The term osteopathy was first used by Andrew Taylor Still. He founded osteopathy in the late 1800s. He was a physician and surgeon of the time. Osteopathy came to Britain in 1913 with one of his students Dr John Martin Littlejohn, and in 1917 he set up the first osteopathic school in the country, the British School of Osteopathy.
However, through some research, I discovered literature showing that long before this period, our forefathers the bonesetters, where achieving some excellent results using the resources of their time. So we know that the art of manual treatment for the aches and ills of the human frame has been practiced for many centuries. Indeed it has been used in China for thousands of years.
As osteopaths we need to understand how the body works. We need to know the normal anatomy and normal physiology. We need to know how the different body systems work together. At this point I would like to ask you to visualise how our body parts work, and therefore recognise how they malfunction. When they go wrong, they hurt.
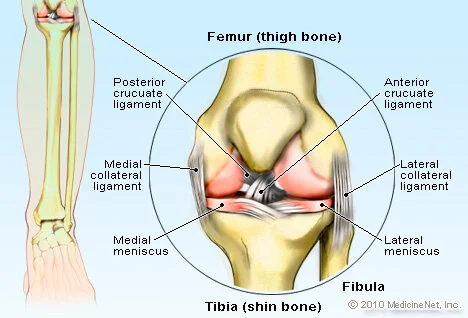
In this example I would like to use the knee joint (see illustration). This is a common joint that hurts. It can hurt for many reasons but the principles are similar. A knee is described as being a hinge joint. So imagine the hinge in a door. Its basic design is to open the door. A knee is designed to bend at the junction between the thigh bone (femur) and the lower leg bone (tibia). You are now immediately aware that a knee can easily be damaged when asked to do anything but bend; it will be damaged for example if you twist it. Common knee injuries are seen on the ski slopes for this reason. To build upon the complexity of the simple hinge joint, imagine the two bones mentioned as having to be held together. This function is carried out by a system of guy ropes (ligaments). These are present on the inside of the joint which cross over (the cruciates) as well as to either side of the bones (the collaterals).
For the first article I chose an unifying topic, osteopathy. All of you receiving this are united by this one common denominator. You may have visited our clinics, you, your horse or pet dog have received osteopathic treatment or are simply interested in what we have to say and have signed up to read our articles.
Now with that image in mind, you can begin to understand how a sudden and violent twist or impact can over-stretch or tear these ligaments, as seen in rugby injuries for example. Now imagine the creaky hinge of an old door. It creaks because the same door has been opened and closed over many years, and it start to wear. This is what happens with an arthritic knee; it's worn and starts to clonk. Even this early on you can begin to apply sensible attitudes to your own body. For example, we all know that a hinge is more likely to wear out quicker if the door is very heavy. The greater the loading on the joint, the more likely the joint will degenerate quickly.
Now the question of usage. We have all seen Dracula films where large and heavy wooden castle doors creak loudly when these same doors are kept shut for a long time. Remember, all moving parts are designed to be kept moving. Just like the door hinge, knee joints that get little use soon stiffen. Moderate and appropriate exercise is the key to minimising pain in the worn knee. Essential structures which allow movement to occur are the muscles. They are effectively your arms shutting the door. The leg muscles provide the activating force for movement to happen. Again, keep the muscles fit and the knee can keep working.
The picture becomes more complex and more fascinating still. For example, muscles need instructions. The instructions come from the mind. Our minds instruct the brain to send messages along the spinal cord, which in turn reaches the nerves that instruct the muscles what to do. But when do we ever need to simply bend the knee? Very occasionally is the answer. We have provisions for this too. For example, most times we bend the knee we tend to need to bend the hip. For this to happen there are two fundamental mechanisms. The first being the main thigh muscle (the quadriceps) crosses both the knee joint as well as the hip joint. The second being they share the same nerve supplies, which explains the mechanism of referred pain. There may be some of you reading this article that were told by an orthopaedic surgeon that your knee pain is actually coming from the hip (referred pain). There are more structures and more mechanisms in the knee joint such as the blood supply and venous return which could be responsible for some swollen veins behind the knee or a large fluid swelling behind it as a result of inflammation and pooling of the fluid behind the knee causing a Baker's Cyst.
The reason for this visual and virtual dissection is to illustrate how we work. We ask you the history of the problem to formulate a working diagnosis, and then, using our hands, we feel for the alteration in the normal anatomy. When presented with a simple clinical presentation, we use specific hands-on techniques to try to re-address the normal function of the moving parts.
This example is uncomplicated. Our work becomes more challenging when we apply this to the person, not simply the anatomical default. We integrate the knee within the leg, which belongs to a person. A person being a complex living mechanism with particular physical demands on the knee and any related emotional complications which may ensue as a result of the injured knee.
This daily detective process occurs with each and every case we see. We need to get to know the person, the lifestyle and the demands placed upon the injured part as well as needing to recognise the physical problem. However, before we start a course of treatment, we need to make sure we do not need to seek the evidence from further testing such as X-Rays or MRI scans, or indeed, the opinion of our colleagues within the medical system. We may need to refer on to a GP for further medical screening, or say, to an orthopaedic surgeon if there are any indicating factors. Our work is not done until we have looked at the whole picture as well as giving advice on rehabilitation where appropriate.
Embracing the whole picture, the whole person both in body and mind, as well as the social demands on the individual person, is the essence of holistic healthcare. Approaching both physical ills and pains of the skeletal structure through the understanding how the body works was as essential in the early years of osteopathy as it is today.
Going back to early osteopathic literature, I would like to share a poignant and still relevant anecdote dating back to the days of Andrew Taylor Still.

“During a diarrhoea epidemic he dealt with many sufferers and his reported success suggests that he was rather more helpful than his medical opponents [he was seen as an outsider by them]. This success was owed to more his philosophy of using no drugs but simple hygiene!”













